
.webp) 1 week ago
7
1 week ago
7
People with diabetes don't have higher gastric volumes than those without diabetes after following standard preoperative fasting instructions, suggested a study from a team of anesthesiologist researchers.
However, an endocrinologist faulted the study in part because the participants appeared to be healthier than typical populations with type 1 and type 2 diabetes. Moreover, the issue is now further complicated by the widespread use of glucagon-like peptide-1 (GLP-1) receptor agonists for the treatment of both type 2 diabetes and weight loss. These drugs, which were introduced after the study's enrollment period, work in part by delaying gastric emptying.
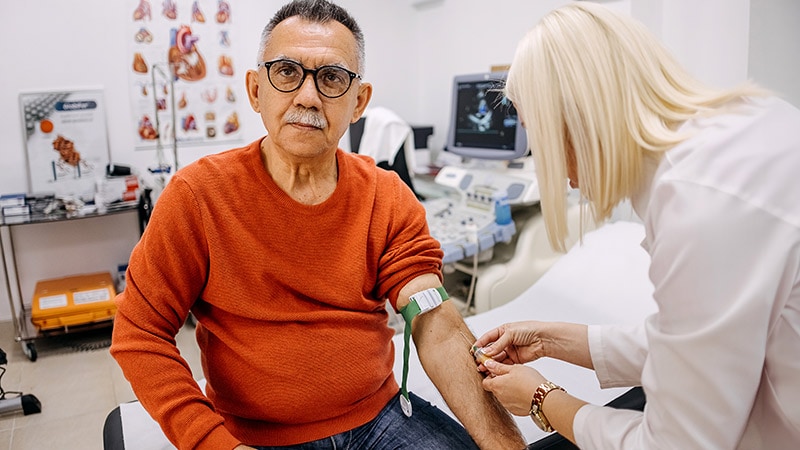
The new data come from a prospective study of 84 people with diabetes (85% with type 2) and 96 without diabetes, all with a body mass index (BMI) < 40, who were undergoing elective surgery. A gastric ultrasound was used to assess their gastric contents after they had followed the standard preoperative fasting guidelines of stopping solids 8 hours prior to the procedure and clearing liquids 2 hours prior.
There was no significant difference between the two groups in gastric volume (0.81 mL/kg with diabetes vs 0.87 mL/kg without) or in the proportion with "full stomach," as designated by the American Society of Anesthesiologists (ASA) guidelines (any solid content or > 1.5 mL/kg of clear fluid), which was seen in 13 with diabetes (15.5%) and 11 (11.5%) without.
Published in Anesthesiology, the findings offer reassurance that different fasting instructions generally aren't needed for people with diabetes in order to minimize the risk for perioperative pulmonary aspiration, lead author Anahi Perlas, MD, professor of anesthesiology and pain medicine at the University of Toronto, Toronto, told Medscape Medical News.
"We never change practice completely based on a single study, but I think in general, based on our findings, that most diabetic patients aren't any different from nondiabetics when it comes to their gastric content after fasting, and our standard fasting instructions seem to be just as effective in assuring an empty stomach."
But she added, "If someone has symptoms of gastroparesis or when in doubt, we can always do a gastric ultrasound exam at the bedside and see whether the stomach is full or empty…it's very quick, and it's not difficult to do."
Expert Identifies Noteworthy Study Limitations
In an accompanying editorial, Mark A. Warner, MD, professor of anesthesiology at the Mayo Clinic in Rochester, Minnesota, said the findings "will be very helpful to anesthesiologists," although he noted that the exclusion of people with a BMI > 40 is a limitation.
However, Michael Horowitz, MBBS, PhD, FRACP, director of the Endocrine and Metabolic Unit at the Royal Adelaide Hospital and professor of medicine at Adelaide Medical School in Adelaide, Australia, disputed the study's conclusions. He noted that the sample was small, and the participants had an average A1c of 7.2%. Fewer than half had microvascular or neuropathic complications. Thus, they were healthier than the general population with diabetes.
"They've picked the wrong group of diabetics," said Horowitz, who specializes in gastrointestinal complications of diabetes. "This is not a group where you would expect a very high prevalence of delayed emptying."
Gastric emptying of solids and liquids varies widely even among healthy people and more so in those with type 2 diabetes. About a third of those with above-target A1c levels have gastroparesis, while those more in the target range tend to have accelerated emptying, he explained.
And regarding the use of gastric ultrasound for those who are symptomatic, Horowitz said, "The relationship of symptoms such as nausea, vomiting, fullness, whatever it may be, with the rate of gastric emptying is weak at best. The association is not simply cause and effect."
Are the Fasting Guidelines Flawed, Regardless of Diabetes Status?
Horowitz also faulted the ASA's 2017 guidance revision for allowing clear liquids to be consumed up to 2 hours in advance of anesthesia because it doesn't distinguish between liquids with and without calories.
"Whether you have diabetes or not, if you are allowed to have a sugar drink up to 2 hours before your operation, the majority of people empty at about 4 kcal/min, so they will still have some of that drink in their stomach," he said. "If you want an empty stomach, the ASA guidelines are wrong."
That explains why the study found relatively high rates of "full stomach" in both groups, 15.5% of those with diabetes and 11.5% of those without, he said.
The GLP-1 Agonist Factor
Although the study didn't address GLP-1 receptor agonist use, Warner did in his accompanying editorial, noting that the drugs' rapid expansion "will likely change how we use perioperative fasting guidelines. With these medications delaying gastric emptying times, we now have another risk factor for pulmonary aspiration to consider when applying fasting guidelines. The inconsistent impact of GLP-1 agonists on gastric emptying, ranging from little to significant, makes it difficult for anesthesiologists to gauge whether or not patients taking GLP-1 agonists are likely to have preoperative gastric liquid or solid contents that could cause subsequent damage if regurgitated."
Gastric ultrasound can be helpful in this situation, Warner wrote. In addition, he endorsed the 2023 ASA guidance, which calls for withholding daily-dosed GLP-1 agonists on the day of the surgery and the weekly formulations for a week. And if gastrointestinal symptoms are present, delay elective procedures.
But Horowitz said those recommendations are likely insufficient as well, pointing to data suggesting that daily liraglutide can delay gastric emptying for up to 16 weeks in about a third of patients. Such studies haven't been conducted by the manufacturers, particularly on the once-weekly formulations, and the ensuing risk for aspiration isn't known.
"The slowing occurs in much lower doses than are used for glucose lowering," Horowitz said. "It is very likely that plasma levels will need to be extremely low to avoid gastric slowing. The current guidelines fail to appreciate this. So, to withhold the short-acting drugs for 1 day is probably wrong. And to stop long-acting drugs for 1 week is almost certainly wrong too."
But as for what should be done, he said, "I don't actually know what you do about it. And no one does because there are no data available to answer the question."
The study received funding from the Physicians' Services Incorporated Foundation and the Canadian Society of Anesthesiologists. Perlas received support for nonclinical time through a merit award from the Department of Anesthesiology and Pain Medicine, University of Toronto, and the Department of Anesthesia and Pain Management, Toronto Western Hospital, University Health Network. She is an executive editor of the journal Regional Anesthesia and Pain Medicine and does consulting work for FujiFilm SonoSite. Horowitz had no relevant disclosures.
Miriam E. Tucker is a freelance journalist based in the Washington, DC, area. She is a regular contributor to Medscape Medical News, with other work appearing in the Washington Post, NPR's Shots blog, and Diatribe. She is on X @MiriamETucker.






















 English (US)
English (US)