
.webp) 2 weeks ago
7
2 weeks ago
7
Women who are considered to be at average risk for breast cancer should have mammograms every other year starting at age 40 years until age 74, according to the latest recommendations from the US Preventive Services Task Force (USPSTF).
In its updated recommendations published today in JAMA, the USPSTF also made an urgent call to address reasons why Black women are more likely to die from breast cancer than are White women and pressed for more research to address persisting questions about how best to screen for cancer in dense breasts, which about 40% of women have. The USPSTF highlighted evidence gaps on the benefits and harms of continuing mammography after age 75 years as well.
The updated USPSTF recommendations were first unveiled last year in a draft version.
In 2016, the task force recommended biennial mammograms for women starting 10 years later, at age 50 years, while stressing a need for clinicians and patients to weigh the risks and benefits of screening for those in their 40s.
The shift to a general recommendation to start at age 40 years is based on a broad review of available data on mammography, including modeling from Cancer Intervention and Surveillance Modeling Network (CISNET).
Alongside the USPSTF report, JAMA published three separate editorials — a reflection of the controversy that these breast cancer screening recommendations often generate.
In one editorial, Lydia E. Pace, MD, MPH, and Nancy L. Keating, MD, MPH, highlighted that though screening earlier will prevent more deaths from breast cancer, it will also lead to more false positive findings and increase rates of overdiagnosis.
Pace and Keating explained that the modeling study commissioned by the USPSTF estimated that screening every 2 years starting at age 40 years would avoid an additional 1.3 breast cancer deaths compared with screening at age 50 years. Among Black women, screening every 2 years starting at age 40 years would avert an extra 1.8 breast cancer deaths per 1000 people screened.
However, the model also found that screening every 2 years starting at age 40 years would lead to more false positive tests — a rate of about 8.5% vs 7.8% for those starting at age 50.
"Given mammography screening's modest benefits, we feel that all women—and particularly those aged 40 to 49 years—should be counseled about the benefits and harms of mammography and supported in deciding whether the balance of benefits to harms fits with their priorities and values," wrote Pace and Keating, who both have specialties in internal medicine.
In a second editorial, Joann G. Elmore, MD, MPH, of UCLA, and Christoph I. Lee, MD, MS, of the University of Washington, Seattle, noted that the revised recommendations "shed light on 2 major issues that demand greater attention: addressing health inequities related to breast cancer outcomes and ensuring benefits for all women amid rapid screening technological advancements."
The UPSTSF's decision to recommend an earlier start age for routine mammography was partly intended to begin to address the fact that Black women are about 40% more likely to die from breast cancer than are White women.
"Despite greater absolute benefits of screening for Black women, the modeling study and systematic review underscore that mammography's benefits (ie, breast cancer deaths averted) are modest for both Black women and the general population," Elmore and Lee wrote.
The editorialists also cautioned against adopting artificial intelligence (AI) support tools too rapidly, criticizing the USPSTF for overlooking this "pressing issue."
"While AI algorithms show promise for enhancing cancer detection, their impact on patient outcomes and the balance between benefit and harms remain uncertain," Elmore and Lee wrote.
In a third JAMA editorial, Wendie A. Berg, MD, PhD, a radiologist at the University of Pittsburgh, Pennsylvania, argued that though the updated recommendations are "an important step forward," they don't go far enough.
Berg, for instance, noted her surprise " to see the USPSTF recommendation only for biennial, rather than annual, screening among women aged 40 to 74 years."
Compared with no screening, annual screening would reduce rates of breast cancer mortality (35.2%) more than biennial (28.4%) screening does among women aged 40-74 years, according to the CISNET modeling that informed the USPSTF's decision.
Plus, Berg noted, regular risk assessments should begin at age 25 years "to identify women at high risk who should start annual MRI screenings."
The American College of Radiology (ACR) offered similar views in a statement, saying the recommendations "do not go far enough to save more women's lives." It urged a more aggressive screening schedule, which starts at age 40 years but occurs annually vs biennially and continues past age 74 years. Like Berg, the ACR advocated for breast cancer risk assessments to begin at age 25 years.
The American Cancer Society also recommended annual mammography screening, starting as early as age 40 years in average-risk women, with high-risk women receiving a breast MRI and a mammogram every year starting at age 30 years.
Ongoing Uncertainties
The USPSTF's 2024 update highlighted persistent evidence gaps in several key areas.
The USPSTF, for instance, highlighted insufficient evidence on the benefits and harms of using digital breast tomosynthesis vs standard mammography for primary screening, the benefits and harms of continuing to screen women who are 75 years or older as well as the benefits and harms of supplemental screening with breast ultrasonography, digital breast tomosynthesis, or MRI in women with dense breasts who had a negative screening mammogram.
In the update, USPSTF also noted that it's still clear what proportion of ductal carcinoma in situ involves lesions detected by screening would not have ultimately caused harm.
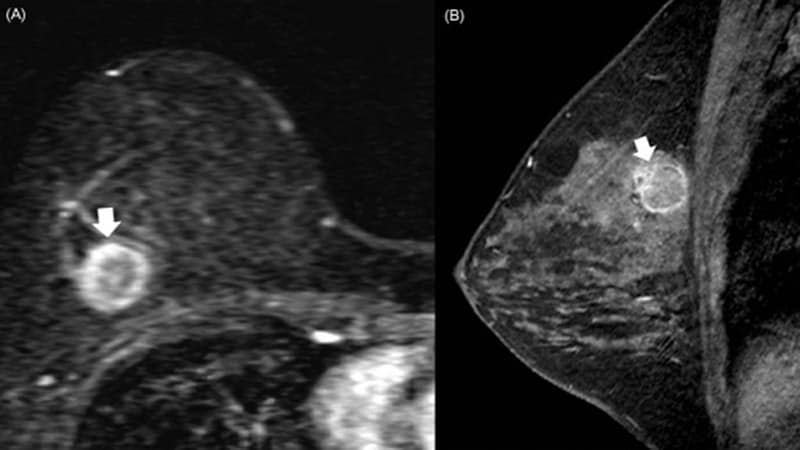
For women with dense breasts, the USPSTF said that "research is needed to help clinicians and patients understand the best strategy for breast cancer screening in women found to have dense breasts," which includes supplemental screening.
Women with dense breasts should still get mammograms, but there is not enough evidence for a blanket statement about which benefit they might get from additional screening, Carol Mangione, MD, past chair of USPSTF, told Medscape Medical News.
"We don't want to send a message that the mammogram doesn't have value in that group, because it does have high value," said Mangione, also chief of the division of general internal medicine and health services research at UCLA Health.
Women with dense breasts should work with primary care clinicians who can take a holistic view of their preferences and needs, allowing them to make an informed choice about additional screening, she said.
"But we can't make a global population choice because we don't have the studies to do that," Mangione said.
Kerry Dooley Young is a freelance journalist based in Washington, DC.























 English (US)
English (US)