
.webp) 3 weeks ago
10
3 weeks ago
10
A 48-year-old man presents to his primary care provider for a routine physical examination. He has a history of hyperlipidemia; he does not have any known heart disease. His pulse is noted to be rapid and irregular, and a 12-lead ECG is obtained.
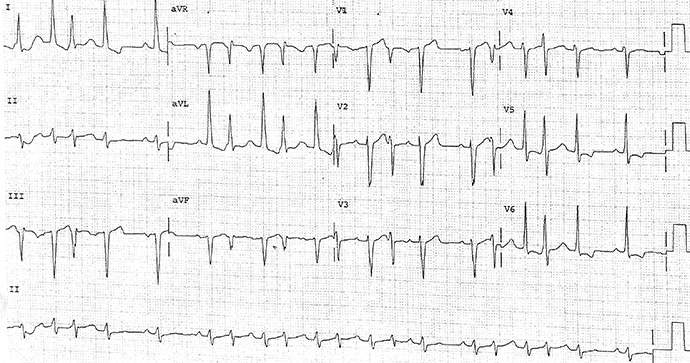
Figure 1. Courtesy of Philip J. Podrid, MD.
The correct diagnosis is normal sinus rhythm with junctional bigeminy (Figure 2).
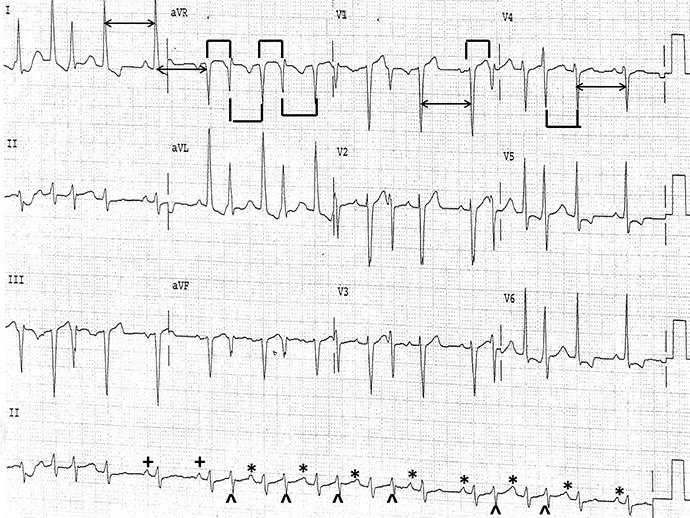
Figure 2. Courtesy of Philip J. Podrid, MD.
Discussion
The rhythm is irregular, but many of the RR intervals are the same: all the long (↔), short (└┘), and intermediate (┌┐) intervals are the same. Hence the rhythm is regularly irregular.
A P wave occurs before the fifth and sixth QRS complex (+) with the same PR interval. These are two sequential sinus complexes. The rate is 75 beats/min. Considering this PP interval, these are regular P waves seen throughout (*). All the PR intervals are the same (0.16 sec). The P waves are positive in leads I, II, aVF, and V4-V6. This is an underlying normal sinus rhythm at a rate of 75 beats/min. The QRS complexes have a normal duration (0.08 sec) and morphology. The axis is very leftward between -30° and -90° (positive QRS complex in lead I and negative in leads II and aVF). This is a left anterior fascicular block.
The QT/QTc intervals are normal (360/400 msec). Following many of the sinus complexes is a premature complex (^) with the same QRS complex morphology and duration, although there is a different amplitude. These complexes are not preceded by a P wave. Hence, they are premature junctional complexes. Because they are not associated with a pause and do not alter the PP interval, they are considered interpolated.
There are periods where every other QRS complex is a premature junctional complex; this is intermittent junctional bigeminy. Therefore, this is not a tachycardia but rather a normal sinus rhythm with interpolated junctional premature complexes in a bigeminal pattern. Junctional complexes often have a different amplitude or axis, as well as T waves because they enter the bundle of His at a different location and are conducted through the His-Purkinje system slightly differently compared with impulses conducted through the atrioventricular node.
Philip Podrid, MD, is an electrophysiologist, a professor of medicine and pharmacology at Boston University School of Medicine, and a lecturer in medicine at Harvard Medical School. Although retired from clinical practice, he continues to teach clinical cardiology and especially ECGs to medical students, house staff, and cardiology fellows at many major teaching hospitals in Massachusetts. In his limited free time he enjoys photography, music, and reading.


























 English (US)
English (US)